-
Organization apps; Feel more in control of your life
This post is a continuation of my series on organization. I’ve been an organization nerd since childhood. When asked what I wanted as a gift, I’d tell people I wanted office supplies so I could “play office.” Now, instead of excitement about new office supplies, I get excited about trying out new productivity apps and […]
-
Getting stuff done: how to organize tasks and stay focused
This is the second post in my series on getting organized. Today we’re focusing on how to prioritize tasks and stay focused until they’re finished. #1 Use a system that reminds you I’m a huge fan of Getting Things Done (GTD). To get a feel for the concept behind GTD, ask yourself, “Does my brain consistently remind […]
-
Organization tips and tricks
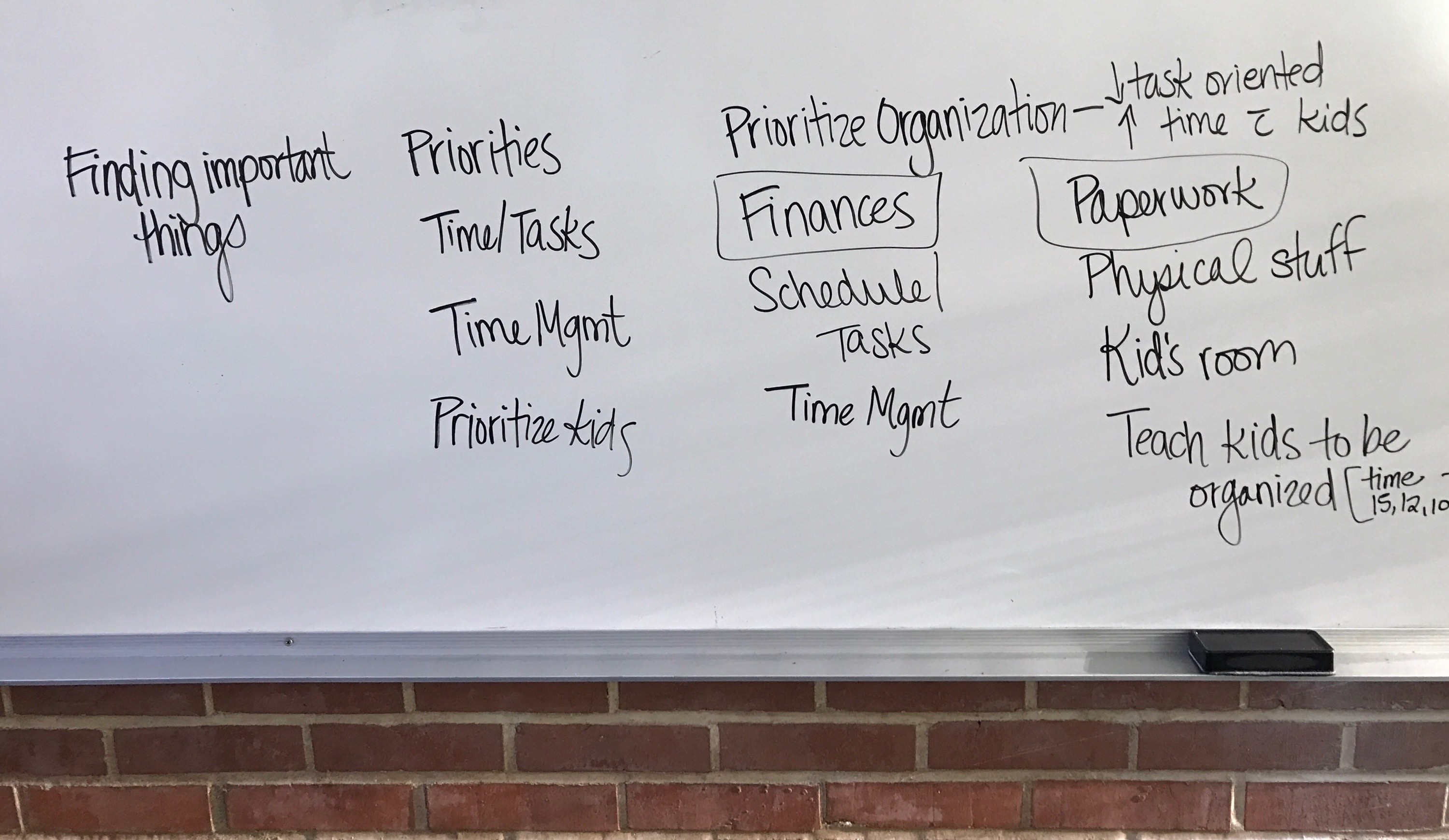
I was recently asked to lead a workshop about organizing. As a self-professed “organization nerd,” I’ve discovered that organization is really about doing whatever works best for you. I see organizing as small adjustments that help people feel like they have a little more power over their physical space and time. So instead of lecturing […]
-
Why I chose nursing
A few years ago I was working late when a co-worker said, “Why are you still here? It’s not like we’re curing cancer.” The reason was simple: it’s in my nature to focus intensely and invest significantly regardless of what I’m doing. This conversation prompted questions like: Am I making a difference in the world? […]
-
If I was my patient, how would I feel?
THEY say “Remember apple, table, coin.” Apple. Table. Coin. I am angry. You would be too. Try not being able to speak. Attempt to communicate and cause only confusion. Try wearing a brief. Sit in your urine and wait. Then in your feces. And to make the indignity worse Allow a stranger to invade your […]
-
Humans not diagnoses; Reflecting on CNA clinicals
This summer I took a CNA class in preparation for nursing school. Here’s what I learned. Our patients are not just diagnosis. They are people. They have a history. Their feelings and experience—both past and present—matter deeply. I can imagine that it becomes easier to see them as tasks to perform instead of people to […]
-
Next stop: nursing school!
Thought I’d post an update on where I’m at with “going back to school and completely changing careers”. I start Nursing School at Wenatchee Valley College in 17 days! It’s a 2-year ADN (Associates of Nursing) degree. As preparation, I completed a CNA course over the summer. I walked into class saying “I’m not sure […]
-
How fats we eat become energy in the body
The farther I get into organic and biochemistry the harder it is to find information that uses minimal jargon, helps me find the big picture amidst thousands of details, and that connects the biochemical concepts with what I’m learning in Anatomy & Physiology. So, I decided to post what I recently learned about how the […]
-
What’s next on my midwifery journey
Hi friends and family! As I shared in September, I am on a journey to become a midwife. I’ve wrestled through the decision on what training and credentialing to pursue and even took a little sidetrack exploring medical school. But I’ve settled on the decision to become a nurse-midwife. This means I’ll become an RN […]
-
Certified Professional Midwife vs. Certified Nurse-Midwife (CPM vs CNM)
REVISED: This blog has been edited based on feedback from the Hearthside Online Midwifery Study Group on Facebook. Once I decided to become a midwife, the next step was determining what type of midwife to become. It was challenging to find thorough information about the different options. I basically could only find a surface-level overview, which I found completely […]